The Precision Frontier: Navigating the Complex Analytical Landscape of Antibody-Drug Conjugate Development
In the rapidly evolving theatre of oncology, few modalities have garnered as much clinical excitement as antibody-drug conjugates (ADCs). Often described as "biological missiles," these sophisticated therapeutics represent a paradigm shift in how we approach targeted cancer treatment. By fusing the extreme specificity of monoclonal antibodies with the devastating lethality of cytotoxic small-molecule payloads, ADCs offer a dual-action mechanism that promises to maximize tumor destruction while minimizing the collateral damage typically associated with systemic chemotherapy.
However, the transition from theoretical elegance to commercial reality is fraught with immense technical, analytical, and regulatory hurdles. As the industry moves toward a new generation of highly complex ADCs, the focus has shifted from simple discovery to the mastery of manufacturing and characterization.
Main Facts: The Anatomy of an ADC
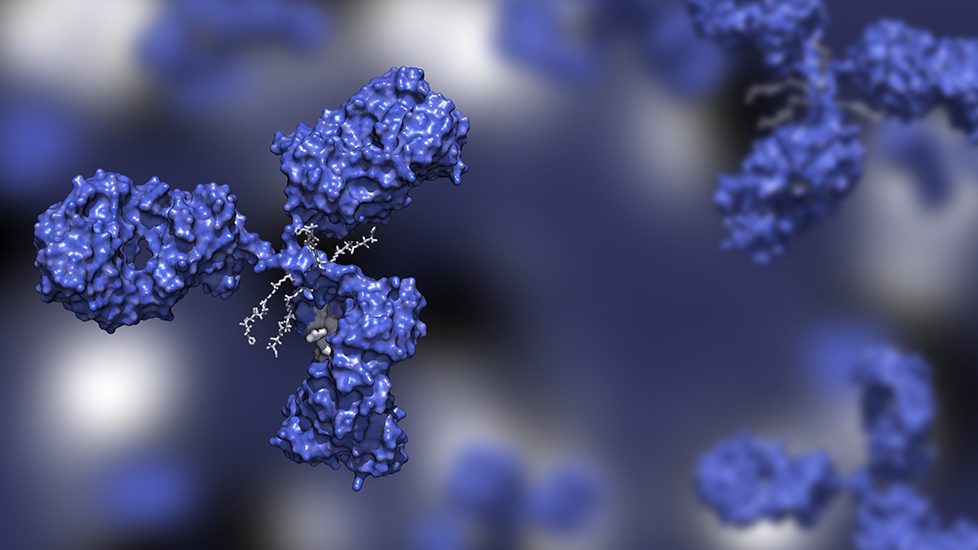
At its core, an ADC is a tripartite construction consisting of three distinct elements:
- The Monoclonal Antibody (mAb): The targeting vehicle, engineered to bind selectively to antigens overexpressed on the surface of tumor cells.
- The Cytotoxic Payload: A potent small-molecule drug, often too toxic for systemic administration, which acts as the "warhead" once internalized by the cell.
- The Chemical Linker: The bridge that tethers the payload to the antibody, designed to remain stable in systemic circulation and release the drug only upon reaching the target site.
The promise of this structure is evident in the recent surge of clinical data. Notably, Phase I findings in platinum-resistant ovarian cancer have provided a proof-of-concept that fuels the field’s current explosive growth. By delivering a targeted dose, ADCs bypass the systemic toxicity that forces many patients to abandon conventional chemotherapy regimens.
Chronology: From Concept to Clinical Transformation
The history of ADCs is a trajectory of iterative refinement. While the foundational concept dates back to the mid-20th century, the first generation of ADCs faced significant setbacks due to linker instability and limited potency.
- 1980s–1990s: The emergence of modern monoclonal antibody technology allowed for the development of the first conjugated agents. Initial efforts were often hindered by non-specific "leaky" linkers that released toxic payloads into the bloodstream, causing significant patient toxicity.
- 2000s: The approval of Mylotarg (gemtuzumab ozogamicin) marked the first major regulatory milestone, despite later voluntary withdrawals and re-approvals due to dosing complexities. This era taught the industry that the "drug-to-antibody ratio" (DAR) was not just a manufacturing metric—it was a critical clinical variable.
- 2010s: The maturation of site-specific conjugation technologies allowed for more homogeneous products, moving away from heterogeneous mixtures that were difficult to characterize and manufacture.
- 2020s–Present: We are now in the "Goldilocks era" of ADC development. With the integration of novel, ultra-potent payloads (such as topoisomerase I inhibitors) and highly stable, cleavable linkers, ADCs are now addressing solid tumors with high efficacy. The focus has moved from "can we build it?" to "can we scale it safely?"
Analytical Challenges: The Complexity of Characterization
The manufacturing of ADCs is arguably more complex than that of any other class of biologics. Because an ADC is a hybrid molecule, it inherits the analytical burdens of both small-molecule chemistry and large-molecule biology.
The Drug-to-Antibody Ratio (DAR)
The DAR is a pivotal determinant of an ADC’s therapeutic window. If the ratio is too low, the therapy is ineffective; if it is too high, the molecule may aggregate, clear too rapidly from the body, or exhibit off-target toxicity. Developers must utilize high-resolution mass spectrometry (HRMS) and hydrophobic interaction chromatography (HIC) to ensure that the distribution of conjugated drug molecules is precise and reproducible.
Linker Stability and Impurity Profiles
The linker is the "Achilles’ heel" of the ADC. If it degrades prematurely, the cytotoxic payload is released into the patient’s system, negating the therapeutic benefit. Analytical teams must perform extensive forced-degradation studies to understand the "release kinetics" of the drug. Furthermore, the synthesis of the linker-payload complex involves highly potent compounds that require specialized containment facilities (OEB 5 classification) to protect operators from sub-microgram exposure.
Conjugation Site Specificity
Modern ADC design focuses on site-specific conjugation—ensuring that the payload is attached to a defined amino acid residue on the antibody. This reduces the heterogeneity of the product, simplifying downstream purification and clinical safety assessments. However, achieving this requires complex bio-conjugation chemistry that must be tightly controlled to prevent the formation of aggregate impurities that could trigger an unwanted immunogenic response in patients.
Supporting Data: The Need for Risk-Based Frameworks
According to recent industry data, the manufacturing failure rate for complex biologics remains disproportionately high compared to traditional small molecules. For ADCs, the risk is compounded by the "hybrid" nature of the supply chain.
- Quality by Design (QbD): Regulatory agencies, including the FDA and EMA, are increasingly demanding that ADC developers implement QbD principles from the earliest stages of development. This involves identifying Critical Quality Attributes (CQAs) and mapping them to specific process parameters.
- Analytical Scalability: A method that works in a benchtop laboratory setting may fail at the 2,000-liter bioreactor scale. Robustness studies are essential to ensure that conjugation reactions remain consistent across manufacturing batches.
- Regulatory Uncertainty: Because ADCs bridge the gap between "drug" and "biologic," they exist in a regulatory grey area. Early interaction with health authorities is critical to aligning on the validation of analytical assays, particularly regarding the quantification of free, unconjugated cytotoxic drug—a key marker of safety.
Official Perspectives: The Collaborative Imperative
Industry leaders emphasize that the future of ADC success lies not just in the lab, but in the conference room. The complexity of these molecules demands a "silo-breaking" approach to development.
"Analytical scientists, process engineers, and regulatory specialists cannot work in isolation," notes one industry analyst. "When you are dealing with a payload that is lethal at low concentrations and an antibody that is sensitive to environmental degradation, the ‘hand-off’ between departments is where the most dangerous risks reside."
Experts advocate for integrated development partners. By working with a single organization that handles the full arc—from the synthesis of the linker-payload to the final drug product formulation—developers reduce the risk of "information loss" that occurs when moving from one vendor to another. This continuity ensures that GMP-compliant protocols are embedded in the project from day one, rather than being "bolted on" at the commercialization stage.
Implications for the Future of Oncology
The implications of mastering ADC manufacturing are profound. As analytical methods become more precise, we can expect to see:
- Dose-Dense Therapies: With better characterization, clinicians will be able to dose patients with greater confidence, potentially achieving curative outcomes in cancers that were previously considered terminal.
- Combination Regimens: ADCs are increasingly being tested in combination with checkpoint inhibitors. The stability and predictability of the ADC are essential for these combination trials to succeed without causing additive toxicity.
- Personalized Payloads: The next frontier is the development of "bespoke" ADCs, where the payload can be swapped out based on the specific mutational profile of a patient’s tumor, effectively creating a "designer drug" platform.
Conclusion: The Path Forward
The "promise" of ADCs is no longer a future prospect—it is a present-day reality backed by clinical success. However, the path to widespread patient access is paved with analytical rigor. Developers who invest in robust, scalable manufacturing processes and foster cross-functional collaboration will be the ones to lead the next wave of cancer care.
As the industry moves forward, the focus must remain on the intersection of biology and chemistry. By treating the ADC not as a drug, but as a complex system of interlinked components, we can ensure that these transformative therapies continue to push the boundaries of what is possible in oncology. The analytical challenges of today are the foundation of the curative therapies of tomorrow.